.png)
Human beings are one of the few animals who have two eyes in front of the face instead on the side and can move both eyes in co-ordination over a wide range instead of having to turn the neck to see. The biggest advantage of this being 'binocular single vision' or 'stereosis/3-D vision'. This improves depth perception or better estimation of distance of objects. The 2-D image seen by each eye has some disparity due to the distance between the two eyes. When these are fused and processed in the brain a three-dimensional (3-D) perception is made. This whole process is a very complex mechanism, and involves constant and controlled movement of the two eye-cameras to maintain focus and keep track of any stationary or moving object.

A squint is a condition where the eyes do not look together in the same direction. Whilst one eye looks straight ahead, the other eye turns to point inwards, outwards, upwards or downwards. Squints are common and affect about 1 in 20 children. You might even spot that your baby has a squint. Most squints develop before preschool age, usually by the time a child is 3 years old. Sometimes squints develop in older children, or in adults. A child with a squint may stop using the affected eye to see with. This can lead to visual loss called amblyopia, which can become permanent unless treated early in childhood. This treatment usually involves patching the better eye, to force the use of the affected eye. Sometimes surgery is needed to correct the appearance of a squint .
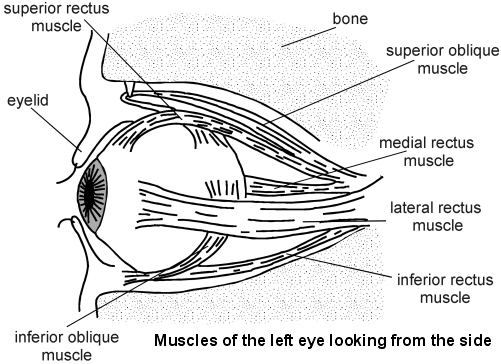
For example, to look to the left, the lateral rectus muscle of the left eye pulls the left eye outwards and the medial rectus of the right eye pulls the right eye inwards towards the nose.
A squint develops when the eye muscles do not work together in a balanced way, so that the eyes do not move together correctly.
The eye movements when tested separately (uniocularly) are called 'ductions' and when both eyes are tested together (binocularly) is called 'versions and vergences'. Normally the two visual axes are parallel when looking at a distance or they meet at the point of regard (the object of attention). In this state the eyes are said to be in alignment (orthophoria or orthotropia). If due to some reason the two visual axes are not aligned to the point of regard, that one eye fixates at the point but the other eye does not, the condition is called strabismus, or heterotropia (squint or cross eyes). The brain does not tolerate double vision or both eyes seeing totally different images and makes all effort to overcome the state of squint by fusional movements and the person may not manifest squint (latent squint or heterophoria). When squint is present at times and controlled at other times it is called intermittent, as against a constant squint.
Yes, squints can be divided into different categories:
In this squint the degree of eye deviation (amount of squint) is equal in all directions of gaze. It has further subtypes viz.
The deviations are more in one gaze than in the other.
Due to involvement (palsy) of one or a group of muscles. The paralysis if incomplete or partial is called paresis:
(i)Neurogenic (nerve or brain defect) due to injury, inflammation, neoplasm, ischemia, diabetes, etc. (ii) Myogenic (muscle defect) due to myasthenia, trauma, inflammation in muscle, thyroid disease, congenital, etc.
Incomitant strabismus is managed by treating the underlying cause. Usually no surgery is indicated in paralytic squint due to systemic causes like diabetes, etc. Following trauma and appropriate attention to various injuries, the patient is followed-up 6 weekly up to 6 months and surgery is indicated only if two or more consecutive 6 weekly follow-ups reveal no change, including diplopia and Hess/Lee charting.
During the waiting period diplopia (double vision) is avoided by covering (occluding) either eye (preferably the nonparalytic eye) or by prisms. Botulinum toxin can be used to temporarily paralyze the antagonist muscle(s).
Surgical treatment is aimed at weakening the ipsilateral antagonist and sometimes also the contralateral antagonist, in addition to strengthening the paralyzed muscle and by transposition of muscles.
 About 5 in 100 children aged 5 years have a squint. It is quite common to notice a brief squint in children when they are tired or daydreaming. Babies sometimes cross their eyes - it is quite normal for this to happen occasionally, especially when they are tired.
About 5 in 100 children aged 5 years have a squint. It is quite common to notice a brief squint in children when they are tired or daydreaming. Babies sometimes cross their eyes - it is quite normal for this to happen occasionally, especially when they are tired.
Some squints are much more obvious than others. You might notice your child has an eye that does not look straight ahead. Another sign of squint is that your child might close one eye when looking at you, or turn or tilts his or her head on one side.
Congenital squint means that the child is born with a squint, or it develops within the first six months of life. In most cases, the eye muscles are not balanced but the reason for this is not known.
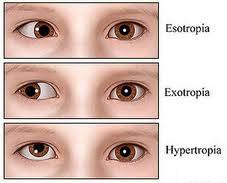
In most cases one eye turns inward. This is called congenital esotropia (sometimes called infantile esotropia). This common type of squint tends to run in some families. However, many children with congenital esotropia have no other family members affected. In some cases the eye turns outwards (congenital exotropia). Less commonly, a squint of unknown cause may result in an upward or downward turn of the eye.
Refractive errors include:Short sightedness(Myopia),Farsightedness (Hypermetropia) and Astigmatism This leads to problems with focusing. These are all conditions that are due to poor focusing of light through the lens in the eye. An astigmatism is a vision problem where the surface of the eye (the cornea) or the lens, is more oval-shaped, rather than round. When the child with a refractive error tries to focus to see clearly, an eye may turn. This type of squint tends to develop in children who are 2 years or older, in particular in children with long sight. The squint is most commonly inward looking (an esotropia).
Whenever strabismus or squint occurs, only one eye can fixate at the object of regard, the other looks elsewhere so that the two fovea (center of retina) receive two different images, creating 'confusion' in the brain. In addition, because of the misalignment of the eyes the same object is perceived as lying at two different positions in space, causing double vision or 'diplopia'.
The brain cannot tolerate confusion or diplopia and it causes the motor system to move the eyes (despite stress) into alignment and convert manifest squint (tropia) to latent squint (phoria). Unusual head posture may be adopted to help the motor system adaptations. The sensory system faces the challenge of squint by sensory adaptations, viz. suppression and anomalous retinal correspondence (ARC). The sensory adaptations are possible only during the stage of plasticity of the neuro-development, that is early childhood, up to 6-8 years of age. If the effect of suppression remains even on closing the other (better) eye amblyopia results.
It is important to diagnose a squint (and amblyopia) as early as possible. Routine checks to detect eye problems in babies and children are usually done at the newborn examination and at the 6- to 8-week review. There is also a routine preschool or school-entry vision check.
Some newborn babies have a mild intermittent squint that soon goes, reducing by 2 months of age and gone by 4 months of age. However, fixed squints are usually permanent unless treated. So, as a guide:
Various tests can be done to check a child's vision. Sight tests can even be done for babies. Tests to find a squint can involve covering and uncovering each eye in turn. This often shows which eye has the squint and how it moves. The pupils of the eye can be checked with a torch, to check they become smaller (constrict) with light and widen (dilate) when the light is removed. An ophthalmoscope is a special torch used to examine the back of the eye (the retina). Very occasionally, if another cause of squint is suspected (other than a congenital squint or one related to refractive errors), a scan of the eye or the brain may be needed.
Treatment typically involves the following:
If a child has a refractive error (long or short sight, for example) then glasses will be prescribed. This corrects vision in the eye. It may also straighten the squinting eye, if the refractive error was the cause of the squint.
In many cases an operation is advised to make the eyes as straight as possible. The main aim of surgery is to improve the appearance of the eyes. In some cases, surgery may also improve or restore binocular vision (this means that the two eyes are working together).
The exact operation that is done depends on the type and severity of the squint. It may involve moving the place where a muscle attaches to the eyeball or, one of the muscles that moves an eye may be shortened. Sometimes a combination of these techniques is used.

Botulinum toxin (also know as Botox) stops muscles from working (it paralyses them). It is used for a variety of conditions where it is helpful to weaken one or more muscles. In recent years, injections of botulinum toxin directly into eye muscles have been used as a treatment for certain types of squint, particularly for squints that turn inward (esotropia). This treatment is an alternative to surgery - but only for certain types of squint.
As a rule, the younger the child is treated, the quicker the improvement in vision is likely to be and the better the chance of restoring full normal vision. If treatment is started before the age of about 7 years then it is often possible to restore normal vision. If treatment is started in older children then some improvement in vision may still occur but full normal vision is unlikely ever to be achieved.
Squint (strabismus) surgery usually greatly improves the straightness of the eyes. Sometimes, even after an operation, the eyes are not perfectly straight. In some cases, two or more operations are needed to correct the squint. Sometimes a special stitch is put in place which can be adjusted later on if further correction is needed.
Squint and amblyopia need early medical attention. Early treatment is very important, especially before 6 years of age. These conditions worsen with advancing age. Squint can be operated at any age and the eyes may be made straight, but squint surgery before 6 years of age carries much better visual results and long-term stability of effect. Squint can be operated in a few months old child.
No, check-up of eyes of a child should be done at least once before one year of age and definitely before admission to school (pre-school age, 4-5 years). The child need not be able to read for the eye surgeon to test the need for glasses or to test for many other eye diseases.
Accommodative squint is to be treated by glasses (or contact lenses) alone. Do not insist for surgery for squint simply because you do not want your child to wear glasses. A qualified eye specialist is the one to decide the best time and mode of treatment. Once the child is older (18 years or more) laser treatment can help accommodative squint by correcting the number of glasses.
Eye muscles are not exercised by looking at a burning candle flame, rotating eyes all around or by walking bare-foot on grass. Proper eye muscle exercises needed in your case should be understood from your doctor or orthoptist.
This is like saying that we will get dependent on our meals to survive. It is a must not an option. Glasses prescribed in childhood are meant to be worn full time. Older children may be given the option of contact lenses or laser treatment. Glasses (or contact lenses) may at times be prescribed for children as young as three months old.
Ptosis is a condition of drooping or falling of the upper eyelid. The sleepy eyes look or drooping may be worse after being awake longer, when the individual's eye muscles are tired. If severe enough and left untreated, the drooping eyelid can cause other conditions, such as amblyopia or astigmatism in young children. This is why it is especially important for this disorder to be treated in children at a young age, before it can interfere with vision development.
Ptosis occurs due to dysfunction of the muscles that raise the eyelid or their nerve supply (oculomotor nerve for levator palpebrae superioris (LPS) and sympathetic nerves for superior tarsal muscle). It can affect one eye or both eyes and is more common in the elderly, as muscles in the eyelids may begin to deteriorate. One can, however, be born with ptosis.
Acquired ptosis is most commonly caused by aponeurotic ptosis. This can occur as a result of senescence, dehiscence or disinsertion of the levator aponeurosis. Moreover, chronic inflammation or intraocular surgery can lead to the same effect. Also, wearing contact lenses for long periods of time is thought to have a certain impact on the development of this condition.
Aponeurotic and congenital ptosis may require surgical correction if severe enough to interfere with vision or if facial looks, cosmetics is a concern. Treatment depends on the type of ptosis and is usually performed by an ophthalmic plastic and reconstructive surgeon, specializing in diseases and problems of the eyelid.
Surgical procedures include:
Non-surgical modalities like the use of "crutch" glasses or special scleral contact lenses to support the eyelid may also be used.
